Investigation of novel SARS-CoV-2 variant
Variant of Concern 202012/01
Technical briefing 6
This briefing provides an update on previous briefings up to 1 February 2021
Summary
There are 4 variants of concern, designated:
• VOC 202012/01 (B.1.1.7), first detected in Kent England is predominant in all regions
and is circulating in multiple countries
• VOC 202102/02 (B.1.1.7 cluster with E484K mutation), first detected in South West
England has been detected in 23 cases
• VOC 202012/02 (B.1.351), first detected in South Africa, 126 case have been
detected in England with evidence of in country transmission. Local testing is
underway and links between cases are being investigated
• VOC 202101/02 (P.1), first detected in Brazil has not been detected in the UK
Nomenclature of variants in the UK
SARS-CoV-2 variants if considered to have concerning epidemiological, immunological or
pathogenic properties are raised for formal investigation. At this point they are designated
Variant Under Investigation (VUI) with a year, month, and number. Following risk assessment
with the relevant expert committee, they may be designated Variant of Concern (VOC).
Variant surveillance overview UK
Data on variants of concern is updated twice weekly online. Total case numbers per VOC as of
10 February 2021 are shown in Table 1.
| England genomic cases 10 February 2021 | ||||
| Variant | Pangolin lineage | confirmed | probable | total confirmed and probable |
| VOC 202012/01 | B1.1.7 | 50,148 | 5,774 | 55,922 |
| VOC 202102/02 | B.1.1.7 with E484K cluster | 23 | 0 | 23 |
| VOC 202012/02 | B.1.351 | 126 | 56 | 182 |
| VOC 202101/02 | P1 | 0 | 0 | 0 |
VOC 202012/01 (B.1.1.7)
This variant was designated VUI 202012/01 (B.1.1.7) on detection and on review re-designated
as VOC 202012/01 (B.1.1.7) on 18 December 2020.
Genomic profile
Lineage defining mutations are shown in Table 2a/b. In addition, VOC 202012/01 has acquired
other mutations in some cases. Mutation counts in the UK dataset are shown in Table 2c.
| S Gene | H69_V70del | 21765_21770del |
| Y144del | 21991_21993del | |
| N501Y | 23063A>T | |
| A570D | 23271C>A | |
| P681H | 23604C>A | |
| T716I | 23709C>T | |
| S982A | 24506T>G | |
| D1118H | 24914G>C | |
| ORF1ab | T1001I | 3267C>T |
| A1708D | 5388C>A | |
| I2230T | 6954T>C | |
| 3675-3677del | 11288_96del | |
| ORF8 | Q27* | 27972C>T |
| R52I | 28048G>T | |
| Y73C | 28111A>G | |
| N Gene | D3L | 28280_2delinsCTA |
| CONFIRMED | All lineage defining non-synonymous changes called as alternate base |
| PROBABLE | At least 5 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
| LOW_QC | Fewer than 5 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
| VOC 202012/01 (B.1.1.7) Spike variants | ||||
| Amino acid change | Total number of instances in VOC 202012/01 (B.1.1.7) (UK data) | 12 November 2020 to 11 December 2020 | 12 December 2020 to 11 January 2021 | 12 January 2021 to 11 February 2021 |
| L18F | 1,844(2.7%) | 8 | 353 | 867 |
| Q677H | 299(<1%) | 0 | 84 | 195 |
| S494P | 514(<1%) | 38 | 210 | 190 |
| Y144F | 207(<1%) | 8 | 120 | 65 |
| A475A | 47(<1%) | 0 | 13 | 27 |
| T678I | 56(<1%) | 0 | 23 | 25 |
| S680F | 36(<1%) | 0 | 12 | 20 |
| E484K | 33(<1%) | 1 | 11 | 19 |
| F490S | 25(<1%) | 0 | 9 | 16 |
| Q677H (alt) | 17(<1%) | 1 | 3 | 13 |
| L455F | 18(<1%) | 1 | 1 | 13 |
| G142V | 21(<1%) | 0 | 8 | 13 |
| G446V | 18(<1%) | 0 | 1 | 12 |
| G142S | 19(<1%) | 1 | 6 | 12 |
| H146Y | 22(<1%) | 0 | 8 | 12 |
| A684V | 27(<1%) | 0 | 9 | 11 |
| R246K | 16(<1%) | 1 | 5 | 10 |
| K150E | 10(<1%) | 0 | 0 | 10 |
| Total VOC 202012/01 (B.1.1.7): 69,568 | ||||
Biological profile
VOC 202012/01 (B.1.1.7) can spread faster than some other SARS-CoV-2 virus variants
currently circulating in the UK. At this time, available evidence suggests that VOC 202012/01
(B.1.1.7) is not strongly associated with antigenic escape from naturally-acquired immunity.
Additionally, VOC 202012/01 (B.1.1.7) is not associated with significant antigenic escape from
vaccine-acquired immunity. VOC 202012/01 (B.1.1.7) mutations do confer escape from a
subset of monoclonal antibodies that target the RBD and NTD.
Transmissibility
The VOC 202012/01 (B.1.1.7) appears to have increased transmissibility compared to
previously circulating variants and has spread rapidly to become the dominant variant in the UK.
Previous transmissibility assessments are available in NERVTAG papers and PHE technical
briefings (secondary attack rate).
Escape from natural immunity
Changes in the genome of B.1.1.7 include changes in the spike glycoprotein. Mutation N501Y
can result in decreased recognition by monoclonal antibodies that bind this epitope. Deletions in
the N terminal domain at residues 69/70, and particularly 144 can results in decreased
monoclonal antibody binding. Since convalescent sera and vaccine-derived antisera are
polyclonal, these mutations usually do not result in consequential loss of serum neutralization.
These mutations could though have large effects on efficacy of monocloncal antibodies used
therapeutically if they specifically target these epitopes.
Severity of disease
Summary data and analyses on severity of disease associated with B.1.1.7 are available:
NERVTAG including 11 February 2021 update on severity.
Epidemiological profile
Lineage B.1.1.7 is dispersed across the UK. Confirmed cases are those identified by whole
genome sequencing. As of 10 February 2021, there were 55,922 confirmed and probable cases
of VOC 202012/01 (B.1.1.7) in England.
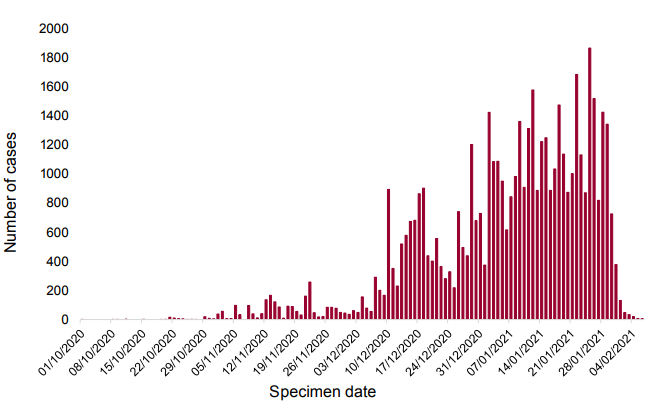
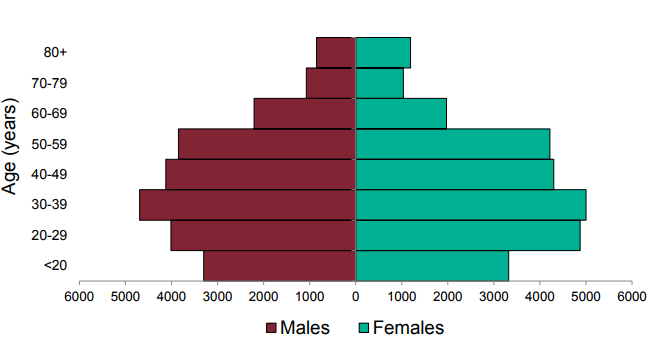
Figure 2. Age sex pyramid of VOC 202012/01 (B.1.1.7) cases, 1 October 2020 to 10 February 2021
| PHE Centre | VOC 202012/01 (B.1.1.7) | All sequenced | ||
| N | % | N | % | |
| East Midlands | 1,545 | 3.1 | 6,808 | 5.2 |
| East of England | 5,934 | 11.8 | 13,445 | 10.3 |
| London | 14,672 | 29.3 | 29,350 | 22.5 |
| North East | 2,202 | 4.4 | 8,194 | 6.3 |
| North West | 10,191 | 20.3 | 28,099 | 21.5 |
| South East | 7,720 | 15.4 | 14,630 | 11.2 |
| South West | 1,468 | 2.9 | 5,126 | 3.9 |
| West Midlands | 3,587 | 7.2 | 11,300 | 8.6 |
| Yorkshire and Humber | 2,471 | 4.9 | 13,657 | 10.5 |
| TBC | 358 | 0.7 | 77 | 0.1 |
| Total | 50,148 | 130,686 | ||
S gene target failure/lineage correlation
The use of S gene target failure in the Taqpath assay as a good proxy for VOC 202012/01
(B.1.1.7) cases has been described in prior technical briefings. This continues to be supported
by current data (Appendix 1). In samples tested with this assay in the Lighthouse Laboratories,
samples with SGTF have predominated since mid December 2020, reaching 95.0% of cases in
the week starting 7 February 2021. Proportions continue to rise by region (Appendix 1).
Hospitalisations
Assessment of hospitalisation is in process.
Deaths
1,072 deaths (within 28 days) of 50,148 confirmed cases have been reported in patients with
VOC 202012/01 (B.1.1.7) as of 10 February 2021.
Cases in individuals who have been vaccinated
Assessment of vaccination data is in process.
International Epidemiology
As of the 10 February 2021 there are 90 countries/territories reporting cases of the UK variants
globally. Of these, 7 report, or there is evidence of community transmission (Canada, Denmark,
Ireland, Netherlands, Slovakia and USA), however for many countries the information available
on the extent of transmission within the country is not always clear.
GISAID (gisaid.org) includes data on sequences available internationally; as of the 12 February
2021 6,982 cases of VOC202012/01 (B.1.1.7) other than those in the UK are listed (Argentina
1, Australia 84, Austria 233, Bangladesh 2, Belgium 579, Bosnia and Herzegovina 1, Brazil 19,
Canada 61, Caribbean 3, Czech Republic 17, Democratic Republic of the Congo 2, Denmark
1,577, Ecuador 7, Finland 41, France 598, Gambia 3, Germany 92, Gibraltar 1, Greece 3, Hong
Kong 4, Hungary 5, Iceland 20, India 32, Iran 1, Ireland 398, Israel 230, Italy 432, Jamaica 4,
Japan 37, Jordan 42, Kuwait 1, Latvia 2, Luxembourg 32, Macedonia 2, Malaysia 2, Mayotte 18,
Mexico 5, Netherlands 486, New Zealand 26, Nigeria 28, North Macedonia 3, Norway 51, Oman
1, Pakistan 2, Peru 1, Poland 10, Portugal 203, Romania 11, Singapore 45, Slovakia 69,
Slovenia 1, South Africa 1, South Korea 13, Spain 468, Sri Lanka 2, St.Lucia 9, Sweden 64,
Switzerland 245, Taiwan 1, Thailand 5, Trinidad and Tobago 1, Turkey 103, UAE 19, USA 522,
Vietnam 1).
VOC 202102/02 (B.1.1.7 cluster with E484K)
Through routine scanning of variation in VOC 202012/01 (B.1.1.7) a small number of B.1.1.7
sequences (33 of 258504 sequences as of 11 February 2021), had acquired the spike protein
mutation E484K. Information suggested more than one independent acquisition event and on
investigation, this forms one predominant cluster and several separate cases or small clusters.
The predominant cluster consists of 17 cases primarily in South West England, 6 elsewhere in
England. This cluster was designated VUI on detection and on review re-designated as VOC
202102/02 (B.1.1.7 cluster with E484K) on 5 February 2021.
Genomic and biological profile
The cluster (VOC 202102/02 (B.1.1.7 cluster with E484K)) has the mutations previously
described for VOC 202012/01 (B.1.1.7) with the addition of E484K in spike gene, L730F in
orf1ab, and A173V, A398T in N gene in all cases. E484K is a mutation of concern with regards
to antigenic change and receptor binding avidity, and is potentially more concerning when
combined with N501Y. E484K is currently the mutation with most evidence of causing antigenic
change. It arises in the presence of convalescent and vaccine-derived antisera. Several
independent studies showing the impact of different antigenic variants have concluded E484K is
among the single mutations with the greatest impact. Secondly, E484K is associated with
increased binding to human ACE2, though it is unclear what impact this has on virus phenotype.
Finally, E484K is associated with multiple variants of concern including the B.1.351 and P.1
lineages, as well as being identified as a long-term adaptation in several different
immunocompromised patient studies. The other mutations specific to this cluster are not
associated with any known phenotypic changes and are not present in other VOCs.
Epidemiological profile
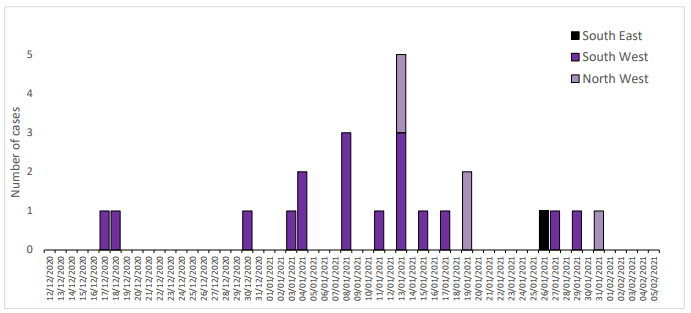
As of 11 February 2021, there were 23 genomically confirmed cases, 17 with an
epidemiological link to Bristol and an additional 6 cases elsewhere in England, with a specimen
date range of 17 December 2020 to 31 January 2021. The epidemiological curve for confirmed
cases is shown in Figure 3. Links between cases are being investigated.
Contact tracing and control measures
Contact tracing is ongoing. Large scale testing in impacted geographies has been implemented
commencing on 7 February 2021. Identification of unlinked cases through Pillar 2 is limited by
sequencing coverage and time lag of at least 2 weeks between isolation and genomic
confirmation. The current number of confirmed cases with this mutation may be underestimated.
Hospitalisations
Of 23 cases, data are available for 18, of which are none were hospitalised following their
infection.
Deaths
Of 23 cases, data are available for 18, of which none have died.
Cases in individuals who have been vaccinated
Of 23 cases, data are available for 18, of which 1 was known to be vaccinated before the onset
of infection (5 days prior).
International Epidemiology
International cases have not been reported.
VOC 202012/02 (B.1.351)
As of 10 February 2021, 126 confirmed and 56 probable cases of VOC 202012/02 (B.1.351,
initially detected in South Africa) have been identified in England. This variant was designated
VUI on detection and on review re-designated as VOC 202012/02 (B.1.351) on 24 December
2020.
Genomic profile
The VOC is lineage B1.351 (first sequence detected in South Africa in October 2020; and in the
UK in December 2020). The complete mutation profile is shown in Table 4.
| Gene | amino_acid>T | actual_nucleotide |
| S Gene | L18F | 21614C>T |
| D80A* | 21801A>C | |
| D215G* | 22206A>G | |
| R246I | 22299G>T | |
| K417N* | 22813G>T | |
| E484K* | 23012G>A | |
| N501Y* | 23063A>T | |
| A701V* | 23664C>T | |
| 242-244del | ||
| ORF1ab | T265I | 1059C>T |
| K1655N* | 5230G>T | |
| K3353R | 10323A>G | |
| 3675-3677del | 11288_96del | |
| ORF3a | Q57H | 25563G>T |
| S171L | 25904C>T | |
| E Gene | P71L* | 26456C>T |
| N Gene | T205I* | 28887C>T |
| CONFIRMED | All lineage defining non-synonymous changes called as alternate base excluding those in red text in Table 4a |
| PROBABLE | At least 4 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base OR at least 5 of the 9 non-synonymous changes indicated by * in the Table 4a |
| LOW_QC | Fewer than 4 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
Biological profile
This variant has 9 mutations associated with transmissibility and antigenic change, of which
E484K and N501Y are most significant. The significance of E484K has been described
previously in this briefing. Variants with the combined N501Y and E484K substitutions have
been shown to have enhanced ACE2 receptor binding.
Escape from natural immunity
Multiple studies with pseudovirus and live virus neutralization assays indicate a significant loss
of antibody binding and neutralization to B.1.351, both with convalescent, as well vaccinederived
polyclonal antisera.
Epidemiological profile
B1.351 is dispersed across the UK in low numbers. Confirmed cases are those identified by
whole genome sequencing; probable cases are COVID-19 cases without sequencing, but who
are contacts of confirmed cases. As of 10 February 2021, there are 126 confirmed cases of
B.351.1 and 56 probable cases. For 18 cases, no travel link has been established indicating
within country transmission. Identification of unlinked cases through Pillar 2 is limited by
sequencing coverage and lag and cases are likely to be an underestimate.
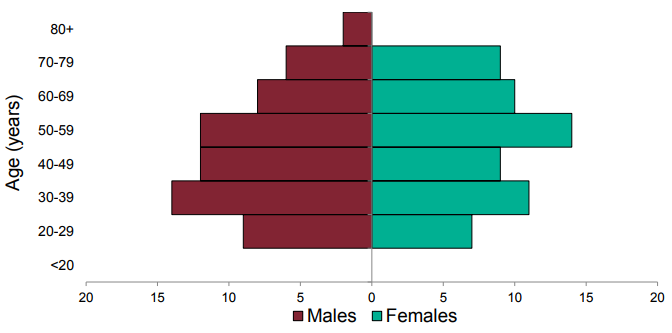
Figure 5. Age sex pyramid of VOC 202012/02 (B.1.351) confirmed cases, 10 December 2020 to 10 February 2021 (3 cases are omitted without age sex data)
| PHE Centre | VOC 202012/02 (B.1.351) | All sequenced | ||
| n | % | n | % | |
| East Midlands | 3 | 2.4 | 6 808 | 5.2 |
| East of England | 26 | 20.6 | 13 445 | 10.3 |
| London | 31 | 24.6 | 29 350 | 22.5 |
| North East | 2 | 1.6 | 8 194 | 6.3 |
| North West | 14 | 11.1 | 28 099 | 21.5 |
| South East | 30 | 23.8 | 14 630 | 11.2 |
| South West | 4 | 3.2 | 5 126 | 3.9 |
| West Midlands | 11 | 8.7 | 11 300 | 8.6 |
| Yorkshire and Humber | 5 | 4.0 | 13 657 | 10.5 |
| TBC | 0 | 0.0 | 77 | 0.1 |
| Total | 126 | 130,686 | ||
Community prevalence studies
REACT study: Altogether 4 VOC 202012/02 (B.1.351) genomes were identified. SARS-COV-2
was detected in 2,282 of 167,642 samples during 6 to 22 January 2021. Of these, samples with
CT values of 34 or less had sequencing attempted; 659 have available sequences, of which
4/659 are VOC 202012/02 (B.1.351) from East of England (2), London (1) and South East (1).
All have sample dates between 7 to 11 January 2021. (Link to Study protocol.)
Office for National Statistics Survey
The ONS survey identified 2 cases of VOC 202012/02 (B.1.351) in samples from December
2020. A total of 1,816 sequences were available for 1 December 2020 to 20 January 2021.
Deaths
1 death (within 28 days) of 126 confirmed cases with data has been reported in patients with
VOC 202012/02 (B.1.351) as of 10 February 2021.
Cases in individuals who have been vaccinated
Vaccination data is being assessed.
International Epidemiology
As of 10 February 2021 there are 40 countries (including the UK) that have reported cases of
this variant globally.
As of 10 February 2021 the epidemiological profile in South Africa is as follows:
• The case incidence is continuing to decrease. Currently, the reported weekly
incidence is 34.2 per 100,000 population. Weekly test positivity has also been
decreasing with current test positivity of 9.7% (testing rates had increased over the
period from around 2 per 1,000 population to over 6 per 1,000 population, although
have declined slightly over the last 2 weeks to 3.5 per 1,000 population).
• The fatality rate is decreasing (the weekly fatality rate is 3.2 per 100,000 population).
• The number of patients in hospital and ICU has also reduced slightly.
Currently, 1,839 COVID-19 patients are in ICU and 11,618 are in hospital.
GISAID (gisaid.org) includes data on sequences available internationally. As of the 12 February
2021 1,130 cases of VOC 202012/02 (B.1.351) are listed (Australia 17, Austria 3, Bangladesh
1, Belgium 59, Botswana 35, Canada 1, Denmark 7, Dominican Republic of the Congo 1,
Finland 2, France 39, Germany 8, Ireland 10, Israel 7, Japan 5, Kenya 6, Luxembourg 2,
Mayotte 23, Mozambique 42, Netherlands 31, New Zealand 7, Norway 1, Panama 1, Portugal
1, South Africa 749, South Korea 1, Spain 2, Sweden 1, Switzerland 23, Turkey 2, UAE 5, USA
7, Zambia 31).
VOC 202101/02 (P.1)
First identified in Japan amongst travellers from Brazil, the P.1 lineage is a descendant of
B.1.1.28. This variant was designated VUI on detection and on review re-designated as VOC
202101/02 (P.1) on 13 January 2021.
Genomic profile
VOC 202101/02 (P.1) is part of a larger international cluster, designated Lineage P.1 (first
sequence noted in GISAID from Brazil in December 2020) and contains 17 unique amino acid
changes, 3 deletions, 4 synonymous mutations, and one 4 nucleotide insertion. The complete
mutation profile is shown in Table 6a.
| Gene | amino_acid>T | actual_nucleotide |
| S Gene | L18F | 21614C>T |
| T20N | 21621C>A | |
| P26S | 21638C>T | |
| D138Y | 21974G>T | |
| R190S | 22132G>T | |
| K417T | 22812A>C | |
| E484K | 23012G>A | |
| N501Y | 23063A>T | |
| H655Y | 23525C>T | |
| T1027I | 24642C>T | |
| orf1ab | - | 733T>C |
| - | 2749C>T | |
| S1188L | 3828C>T | |
| K1795Q | 5648A>C | |
| - | 11288_96del | |
| - | 12778C>T | |
| - | 13860C>T | |
| E5665D | 17259G>T | |
| orf8 | E92K | 28167G>A |
| - | 28263insAACA | |
| N Gene | P80R | 28512C>G |
| - | 28877A>T | |
| - | 28878G>C |
Red text indicates acquisition in subset of isolates within the lineage, non-variant defining
mutations. Blue text indicates mutations present in the lineage but also observed in other
isolates in lineage B.1.1.28, these are not included in the variant definition. Indels (shaded in
orange) are not currently included in variant definitions.
| CONFIRMED | All lineage defining non-synonymous changes called as alternate base |
| PROBABLE | At least 5 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
| LOW_QC | Fewer than 5 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
Biological profile
This variant has mutations associated with both transmissibility and antigenic change including
several in common with the B.1.351 lineage (N501Y, E484K and K417N/T). The significance of
E484K has been described previously in this briefing.
Transmissibility
P.1 has been a been identified in Manaus, Brazil which experienced a rapid growth in numbers
of COVID hospitalisations. Variants with the combined N501Y and E484K substitutions have
been shown to have enhanced ACE2 receptor binding. Increased transmissibility is biologically
and epidemiologically plausible, but at this time there is insufficient evidence to confirm or refute
this. The frequency of such variants within the Brazilian population is difficult to assess.
Re-infections in healthcare workers have been reported in Brazil.
Epidemiological profile
There are no cases in the UK as of 10 February 2021
International Epidemiology
As of 10 February 2021, cases of VOC 202101/02 (P.1) have been reported in 11
countries/territories. 3 countries have reported cases of a Brazilian variant additional information
is awaited to clarify if this is with VOC 202101/02 (P.1).
GISAID (gisaid.org) includes data on sequences available internationally. As of the 12 February
2021 91 cases of VOC 202101/02 (P.1) are listed (Brazil 62, Colombia 9, Faroe Islands 1,
France 3, Italy 3, Japan 6, Netherlands 2, Peru 1, South Korea 1, USA 3).
Diagnostics
Lateral flow devices
Tested lateral flow devices detect VOC 202012/01 (B.1.1.7) and VOC 202012/02 (B.1.351)
when assessed in a laboratory setting using variant virus materials.
Testing of VOC 202102/02 (B.1.1.7 with E484K) and VOC 202101/02 (P.1) are pending
availability of virus material.
qPCR/Molecular amplification testing
A pathway is being established by MHRA to provide continued assurance of performance for
diagnostic devices in use in the UK. This includes a process of analytical evaluation by PHE
and NHSE, where appropriate, to formally test the impact on detection, of variants of
concern, by specific products used for clinical diagnostics.
Appendices
Appendix 1. SGTF Correlation
One S gene mutation in VOC 202012/01 (B.1.1.7) causes deletion of amino acids 69 and 70
(Δ69-70), with a reproducible S gene target failure (SGTF). This is detected by the
ThermoFisher TaqPath assay used in UK lighthouse laboratories (see Technical Briefing 1),
‘TaqPath laboratories.’
This coincidental occurrence provides a good proxy for monitoring trends in VOC 202012/01
(B.1.1.7). SGTF correlates almost perfectly with presence of Δ69-70. Considering 49,945
tested pillar 2 samples where we know both the sequence and the SGTF status, 99.6% of Δ69-
70 sequences (27,001 of 27,099) are SGTF, compared to 0.04% of sequences without the
deletion (10 of 22,846).
Because Δ69-70 has arisen multiple times, and SGTF is a proxy for any lineage with that
mutation, the utility of SGTF as a proxy for VOC 202012/01 varies over time and region. Table 7
shows, for all pillar 2 sequences, the weekly proportion of Δ69-70 sequences that were
confirmed to be VOC 202012/01 (B.1.1.7). Table 8 shows the proportion of Δ69-70 that is the
VOC 202012/01 (B.1.1.7) in England since 21 December 2020, broken down by region. It is
now over 99% in all regions of England. The numbers in these tables are based on sequenced
samples, some of which may have come from the same individual (this effect is likely to be
small).
| Week beginning | Percentage VOC of all Δ69-70 | Number of pillar 2 Δ69-70 sequences |
| 2020-10-12 | 3% | 116 |
| 2020-10-19 | 15% | 220 |
| 2020-10-26 | 29% | 156 |
| 2020-11-02 | 64% | 399 |
| 2020-11-09 | 81% | 711 |
| 2020-11-16 | 88% | 805 |
| 2020-11-23 | 93% | 390 |
| 2020-11-30 | 95% | 433 |
| 2020-12-07 | 98% | 2,712 |
| 2020-12-14 | 99% | 4,300 |
| 2020-12-21 | 99% | 2,407 |
| 2020-12-28 | 99.7% | 5,070 |
| 2021-01-04 | 99.7% | 5,621 |
| 2021-01-11 | 99.9% | 7,473 |
| 2021-01-18 | 99.8% | 6,088 |
| 2021-01-25 | 100% | 1,222 |
| Region | Percentage VOC 202012/01 (B.1.1.7) of all Δ69-70 | Number of Pillar 2 Δ69-70 1 to 31 January 2021 |
| East Midlands | 99.9% | 669 |
| East of England | 99.9% | 2095 |
| London | 99.8% | 4819 |
| North East | 100% | 871 |
| North West | 99.8% | 6615 |
| South East | 99.6% | 2875 |
| South West | 99.9% | 671 |
| West Midlands | 99.6% | 2100 |
| Yorkshire and the Humber | 99.6% | 1283 |
Surveillance of SGTF, as a proxy for VOC 202012/01 (B.1.1.7), is based on positive tests
reported by 3 lighthouse laboratories that use the Thermo Fisher TaqPath RT-PCR, and
for which CT values are low enough to classify if the S gene is detectable. Specifically,
positive tests with CT values >30 for any gene target are excluded. SGTF is defined as a
positive test with CT values <=30 for the N and ORF1ab genes and an undetectable S
gene. S gene positive is a positive test for which all 3 gene targets (N, ORF1ab, S) have
CT values <=30.
Samples with SGTF have predominated since mid-December 2020, reaching 95.9% of
cases in the week starting 4 February 2021 (Figure 6). All regions in England have
reached >93% SGTF in the most recent week (Figure 7). Total cases detected using the
TaqPath assay have also been declining since the first week of 2021, reflecting the
general decline in case rates across England.
Figure 6. Weekly number and proportion of England Pillar 2 COVID-19 cases with SGTF among those tested with the TaqPath assay and with S gene detection results (3 September 2020 to 10 February 2021)
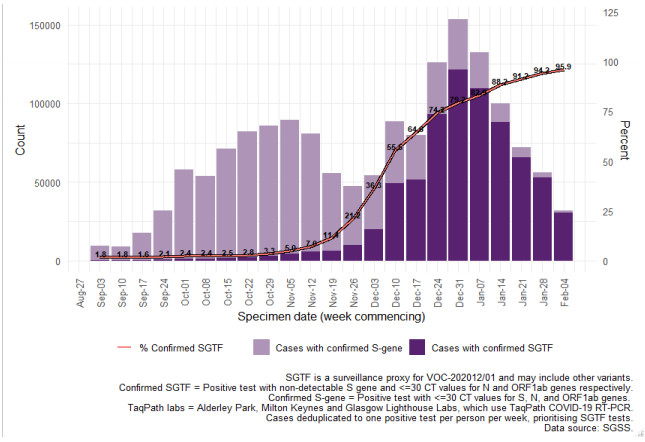
Figure 7. Weekly number and proportion of England Pillar 2 COVID-19 cases with SGTF among those tested with the TaqPath assay and with S gene detection results, by region of residence (3 September 2020 to 10 February 2021)
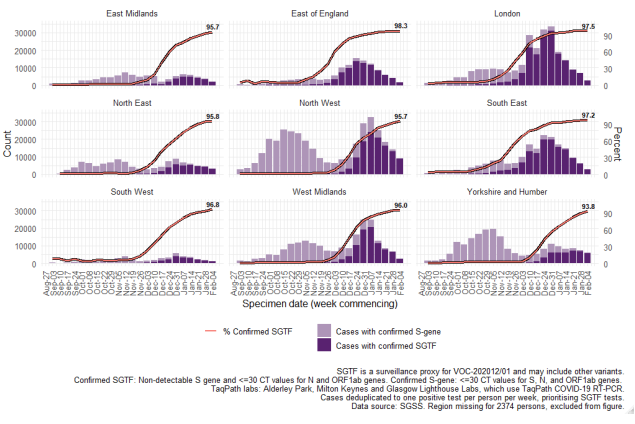
Data on coverage of TaqPath laboratories testing and numbers/proportions of cases with SGTF are shared daily with Local Authorities (Sunday to Friday) on the COVID-19 PHE Local Authorities Report Store (Sharepoint).
Appendix 2 – Variant case definition validation
To determine if case definitions for VOC 202012/02 (B.1.351) are sufficiently sensitive, an
analysis was undertaken. The current definition includes 2 different ‘probable’ definitions,
outlined in Table 9. The amino acid and nucleotide substitutions characterising the variant
are shown in Table 10
| Category | Definition |
| CONFIRMED | All lineage defining mutations (not in red text in Table 10) called as alternate base. |
| Probable 1 | At least 4 lineage defining mutations (not in red text in Table 10) called as alternate base and all other lineage defining positions N or mixed base. |
| Probable 2 | At least 5 of the 5 mutations (marked with * in Table 10) called as alternate base with any combination of other bases. |
| Low Quality | AFewer than 4 lineage defining mutations called as alternate base, and all other lineage defining positions N or mixed base. |
| Gene | Amino_Acid>T | Actual_Nucleotide | Note |
| S Gene | L18F | 21614C>T | not lineage defining |
| D80A* | 21801A>C | ||
| D215G* | 22206A>G | ||
| R246I | 22299G>T | not lineage defining | |
| K417N* | 22813G>T | not lineage defining | |
| E484K* | 23012G>A | ||
| N501Y* | 23063A>T | ||
| A701V* | 23664C>T | ||
| ORF1ab | T265I | 1059C>T | nsp2T85I |
| K1655N* | 5230G>T | nsp3K837N | |
| K3353R | 10323A>G | nsp5K90R | |
| ORF3a | Q57H | 25563G>T | |
| S171L | 25904C>T | ||
| E Gene | P71L* | 26456C>T | |
| N Gene | T205I* | 28887C>T |
Two data sets were included, the COG-UK genomes, and the GISAID dataset. Analysis
with the COG-UK data set identified 110 confirmed UK VOC 202012/02 (B.1.351)
genomes. Analysis using the GISAID data identified 463 international confirmed genomes
(UK data not included). Table 11 shows the number of sequences in each category when
the current probable 1 definition is used (no non-variant nucleotides NVN, sometimes
referred to as wild-type, at VOC defining positions) compared to allowing one or 2 NVN
calls at any of the positions.
| A Definition | Allowing 0 NVN | Allowing 1 NVN | Allowing 2 NVN |
| Both Probable | 38 | 43 | 46 |
| Probable 1 Only | 13 | 13 | 14 |
| Probably 2 Only | 8 | 3 | 0 |
| Total Probable | 59 | 59 | 60 |
| B Definition | Allowing 0 NVN | Allowing 1 NVN | Allowing 2 NVN |
| Both Probable | 96 | 259 | 278 |
| Probable 1 Only | 5 | 5 | 5 |
| Probably 2 Only | 190 | 27 | 8 |
| Total Probable | 291 | 291 | 291 |
Spike drop out and mutations or bases of poor quality data impact variant assignment
using both probable 1 and 2 definitions. Analysis shows probable 1 definition detects
sequences that the probable 2 definition does not, because of uncalled nucleotides in the
genomes. Probable 1 definition enables variant assignment of lower QC VOC 202012/02
(B.1.351) sequences. Conversly, there are genomes that are detected using the probable
2 definition only, potentially due to reversions at some of the lineage defining positions.
Currently the low-quality definition does not allow for NVN calls and therefore will not
detect genomes that include data omissions, and partially meet the probable 2 definition.
Therefore both definitions must be used for variant assignment. Low quality genomes
currently undergo a manual review to determine whether they are considered likely to be
VOC 202012/02 (B.1.351) genomes and public health action is required. Therefore, it is
recommended that the low-quality definition is expanded to capture these genomes. Both
probable definition 1 and definition 2 must continue to be used to enable maximum
assignment of variants in addition to manual check of low-quality sequences.
Data sources
Data used in this investigation is derived from the COG-UK dataset, the PHE Second
Generation Surveillance System, NHS Test and Trace, the secondary uses service (SUS)
dataset and Emergency Care Data Set (ECDS).
Variant Technical Group
Organisations
This group includes representation from the following organisations: PHE, DHSC, BEIS,
Wales NHS, PHScotland, NHS Scotland, Health and Social Care Northern Ireland,
Imperial College London, London School of Hygiene and Tropical Medicine, University of
Birmingham, University of Cambridge, University of Edinburgh, University of Liverpool, the
Wellcome Sanger Institute.
Additional contributions
Additional contributions were received from REACT-1 study (Steven Riley, Oliver Eales
and Paul Elliott on behalf of the REACT Study Investigators, Imperial College London).
Acknowledgements
The authors are grateful to those teams and groups providing data for this analysis,
including: the Lighthouse Laboratories, COG-UK, the Wellcome Sanger Institute, the PHE
Epidemiology Cell, Contact Tracing, Genomics and Outbreak Surveillance Teams.
Published February 2021
PHE gateway number: GW-1934